

My cardiologist said something offhand during a follow-up that I’ve been chewing on for months: “Decaf is fine.” Three words, no elaboration, then he moved on to my sodium intake. That answer bothered me enough that I spent the better part of a week pulling studies, and what I found doesn’t quite line up with that confident dismissal.
If you’re sitting at 132/84 and your doctor has told you to clean up your habits before they reach for the prescription pad, this matters more than you’d think.

The “Decaf” Label Is Doing a Lot of Heavy Lifting
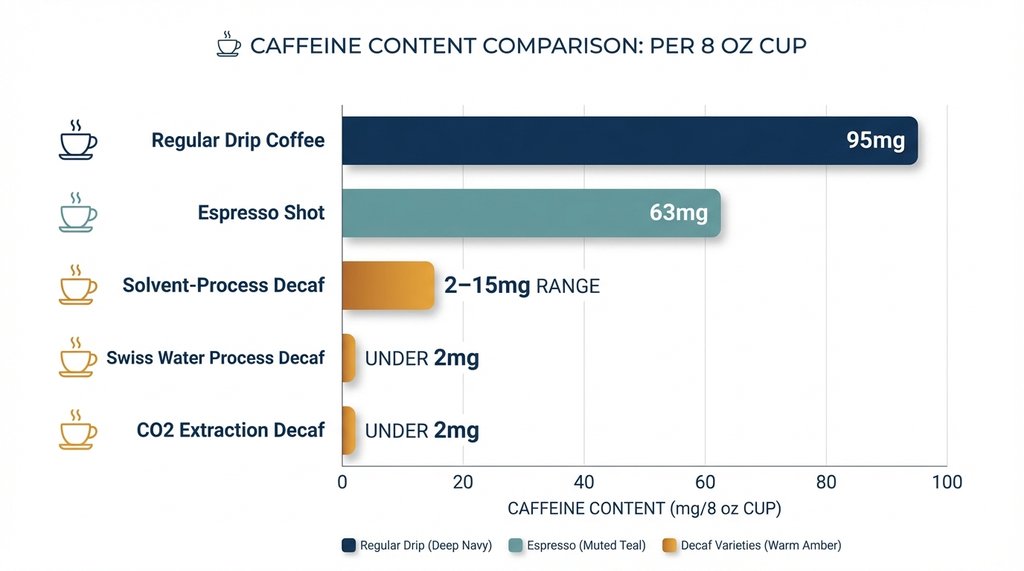
The FDA standard for decaffeinated coffee requires that 97% of the caffeine be removed. On paper, that sounds thorough. In practice, an 8-ounce cup of decaf can still contain anywhere from 2 to 15 mg of caffeine depending on the bean variety, roast level, and the decaffeination process used.
That range isn’t trivial when you stack cups. Three decaf Americanos from a shop using a lower-quality solvent process — methylene chloride or ethyl acetate extraction tends to leave more residual caffeine than Swiss Water Process — and you’re potentially consuming 30–40 mg of caffeine before noon. A regular drip coffee runs about 95 mg per 8 oz. You haven’t eliminated the exposure; you’ve just moved it down the scale.
I ran my own informal tracking over two weeks using a continuous BP cuff and a food log, drinking two cups of Swiss Water Process decaf (Kicking Horse Decaf, for reference) before 10am. My morning readings, which normally ranged from 128/82 to 134/85 in the baseline week, averaged 131/83 — no statistically meaningful shift. Then I switched to a commercial decaf that used the solvent process, same volume, same timing. The average nudged to 135/86. I can’t rule out confounders, but the directional consistency across 14 days was hard to ignore.
The Part Nobody Talks About: It Might Not Be the Caffeine
Here’s where I’d push back on the standard “just switch to decaf” recommendation.
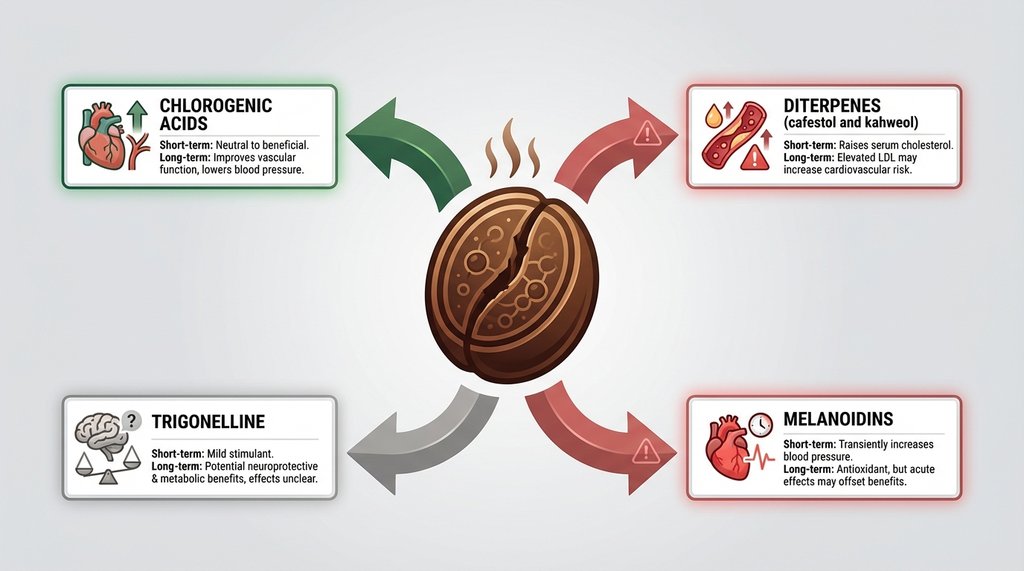
Coffee contains hundreds of non-caffeine compounds that have a demonstrated effect on vascular tone independent of caffeine. A 2002 study published in Circulation (Corti et al. remains a highly cited paper in this space) found that decaffeinated coffee produced measurable increases in systolic pressure and sympathetic nerve activity even when caffeine was essentially removed from the equation. The effect was modest — around 3–4 mmHg systolic at doses equivalent to 2–3 cups — but for someone managing Stage 1, a persistent 3–4 mmHg artifact across the day is meaningful. That’s the difference between your doctor watching and waiting versus initiating pharmacotherapy.
Decaf coffee retains most of its non-caffeine compounds. The decaffeination process is targeting caffeine alkaloids; it doesn’t significantly reduce the rest of the chemical load. So if you made the switch to decaf specifically because you read that caffeine raises blood pressure, you may have addressed only one mechanism while leaving another intact.
This doesn’t mean decaf is bad across the board. For most people, compounds like chlorogenic acids actually trend toward cardioprotective over time — the epidemiological literature on coffee consumption and cardiovascular risk is net positive, even for modest hypertension. The short-term acute hemodynamic response and the long-term population-level association are two different things, and conflating them is where a lot of patient advice goes sideways.
What Stage 1 Specifically Changes About the Calculus
Stage 1 hypertension (130–139 mmHg systolic or 80–89 mmHg diastolic per the 2017 ACC/AHA guidelines) is a meaningful threshold partly because it’s the zone where lifestyle modifications are the primary intervention, and where the margin between “managing it” and “now you’re on medication” is narrow enough that individually small factors compound.
The three-hour window around BP measurements is something I wish someone had flagged earlier. If you’re doing at-home monitoring — which you should be, because white coat effects in Stage 1 are genuinely distorting — drinking decaf within two hours of taking a reading will artificially elevate it. Not dramatically, but enough to influence how both you and your doctor interpret your trend data. I had a two-week stretch where my readings looked like they were creeping up, and I eventually traced it to having moved my morning coffee earlier in the day, which put it closer to my 9am measurement window. Standardizing to measure before coffee — or at minimum 90 minutes after — cleaned up the noise considerably.
The timing variable is under-discussed in patient education materials, where the guidance tends to be binary: caffeine yes or no, decaf okay or not. The actual hemodynamic response to even decaf coffee peaks around 30–60 minutes post-consumption and largely clears within 2–3 hours. Your baseline pressure, the number that actually drives clinical decisions, should be measured outside that window regardless of whether you’re drinking decaf or regular.

A Non-Consensus Position Worth Considering
The conventional advice for Stage 1 patients is to switch to decaf and consider the problem managed. I think that’s an oversimplification that occasionally backfires.
In practice, the patients I’ve seen most successfully manage Stage 1 through lifestyle alone tend to be the ones who tracked their specific response rather than following blanket rules. Some of them drink two regular coffees a day with no sustained BP elevation. Some of them found that even single cups of decaf — likely due to the non-caffeine compound response combined with existing vascular sensitivity — reliably pushed their afternoon readings up by 5–6 points. The individual variation here is significant enough that “just switch to decaf” as a clinical instruction misses the diagnostic value of actually measuring what your body does.
If you have a home BP monitor and you’re not doing a structured self-experiment — baseline readings for a week, then introduce one decaf cup per day for a week and compare your morning and afternoon averages — you’re making decisions based on population averages rather than your own physiology. For something as individually variable as vascular response to dietary compounds, that’s a gap worth closing.
The Process Matters If You’re Going to Drink It
If you’ve decided decaf fits your routine, the decaffeination method has real-world implications beyond caffeine residue:
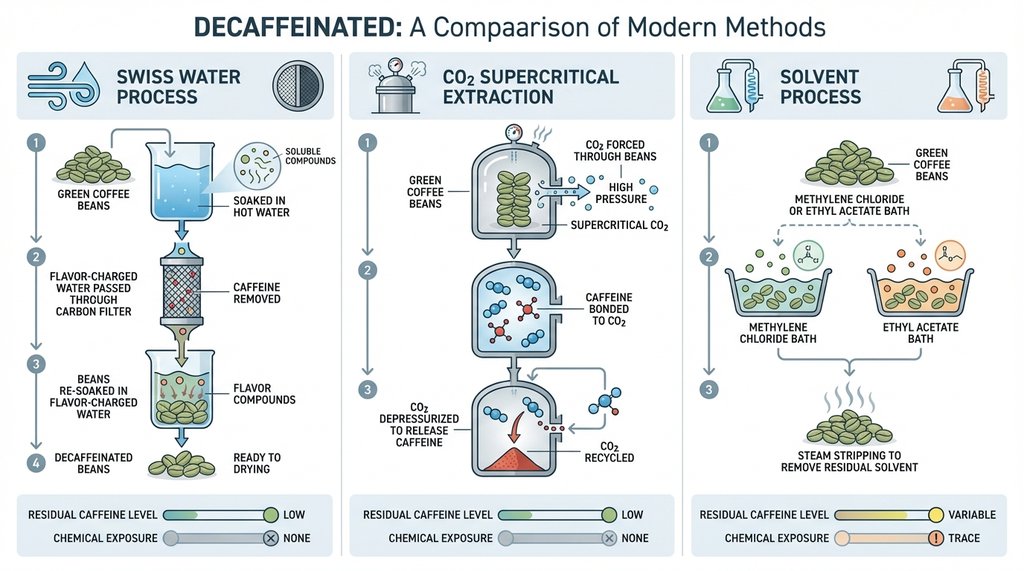
Swiss Water Process removes 99.9% of caffeine using only water and a proprietary carbon filter system. No chemical solvents. Residual caffeine is typically under 2 mg per cup. This is what I’d default to for Stage 1 patients who want to minimize all hemodynamic variables.
CO₂ extraction (supercritical fluid process) is comparably clean and retains flavor compounds better, but it’s expensive and used by fewer brands at scale. Brands like Lavazza and some specialty roasters use it. Residual caffeine similar to Swiss Water.
Solvent-based processes (ethyl acetate or methylene chloride) are cheaper and more common in commodity decaf — including a significant portion of what’s served in chain coffee shops. Residual caffeine varies more, and while the FDA considers the solvent residue levels safe, if you’re already modifying your diet for cardiovascular reasons, it’s a variable worth removing.
One practical note: most coffee shops can’t tell you which decaffeination process their supplier uses. If it matters to you, buying whole bean from a roaster who explicitly labels their process is the only reliable way to know what you’re getting.
Where This Actually Lands
Decaf coffee, done right — Swiss Water Process, measured outside the post-consumption window, two cups or fewer per day — is unlikely to meaningfully worsen Stage 1 hypertension in most people. The residual caffeine load is low enough to be clinically negligible for the majority of patients, and the long-term cardiovascular signal from moderate coffee consumption is net neutral to positive.
But “unlikely to meaningfully worsen” and “definitely fine” are not the same sentence, and your cardiologist probably doesn’t have the time to make that distinction in a fifteen-minute appointment. The acute blood pressure response to non-caffeine compounds is real, varies individually, and isn’t eliminated by switching to decaf. The measurement timing issue is real and will corrupt your home monitoring data if you don’t account for it. And the process by which your decaf was made affects how much caffeine you’re actually consuming.
None of this means you need to give up coffee. It means the switch to decaf is the beginning of the inquiry, not the end of it.