

My third trimester client sent me a photo of her “safe” coffee order last Tuesday — a 20oz cold brew from a regional chain, half-caff. She was proud of herself. I pulled up the chain’s nutritional data and the number staring back at me was 214mg. In one cup. Before 9am.
That’s the problem with caffeine math during pregnancy: the 200mg limit is well-established, the anxiety around it is real, but the actual numbers attached to specific drinks are shockingly misunderstood — by patients, by baristas, and honestly, by a lot of clinicians who should know better.

The 200mg Number and What It Actually Represents
ACOG hasn’t changed its position since it landed on 200mg/day back in 2010, and heading into 2026, that figure remains the clinical consensus ceiling. The NHS holds the same line. What often gets lost in the translation to daily life is that 200mg is a limit, not a target — it’s the threshold below which available evidence doesn’t demonstrate increased risk of miscarriage or fetal growth restriction, not a recommended intake.
That distinction matters when someone asks me “can I have a coffee?” because the answer depends entirely on which coffee we’re talking about. A single-shot latte and a large pourover from a specialty roaster are both “a coffee.” One of them eats 30% of the daily budget. The other blows through it entirely.
Espresso: The Most Misread Entry on the Menu
A standard double espresso — two shots, 60ml — comes in at roughly 120-140mg of caffeine depending on the roast and extraction variables. Single-origin light roasts are often assumed to pull higher than dark roasts because of a misconception that caffeine degrades during the roasting process, but caffeine is actually stable at roasting temperatures; higher caffeine at specialty shops is typically due to larger doses of coffee grounds. I’ve seen third-wave shops pulling singles that measure out to 85mg per shot on a calibrated refractometer setup, which upends the assumption that “just an espresso” is automatically the conservative choice.
The practical figure to work with: 63mg per shot as a conservative baseline, knowing it can run higher at specialty shops using lighter roasts with longer extraction times.
A cappuccino or flat white built on a single shot sits around 63mg. A standard latte with two shots is 120-140mg. That’s manageable. The problem arrives with the third shot that baristas will add automatically if you order anything in a large size at most chains — that’s when you’re casually at 180-200mg from one drink before accounting for anything else consumed that day.

Filter Coffee: The Format Where Volume Does the Damage
An 8oz drip coffee from a home machine brewed at standard ratios — roughly 10g of grounds per 6oz of water — lands around 95-120mg. That sounds fine. The issue is that nobody actually drinks 8oz. The standard American coffee mug is 12oz. Many travel mugs are 16oz. When I ask patients to measure out what they’re actually pouring, the number they’re drinking before they leave the house is closer to 150-180mg for “one cup.”
This is the format where I’ve seen the most clinical miscalculation. A patient will say “I only drink one cup of coffee in the morning” and technically be over the 200mg limit if she’s filling a standard 16oz travel mug from a drip machine. The math isn’t complicated; the problem is that the reference measurement (8oz) doesn’t match any vessel currently in common use.
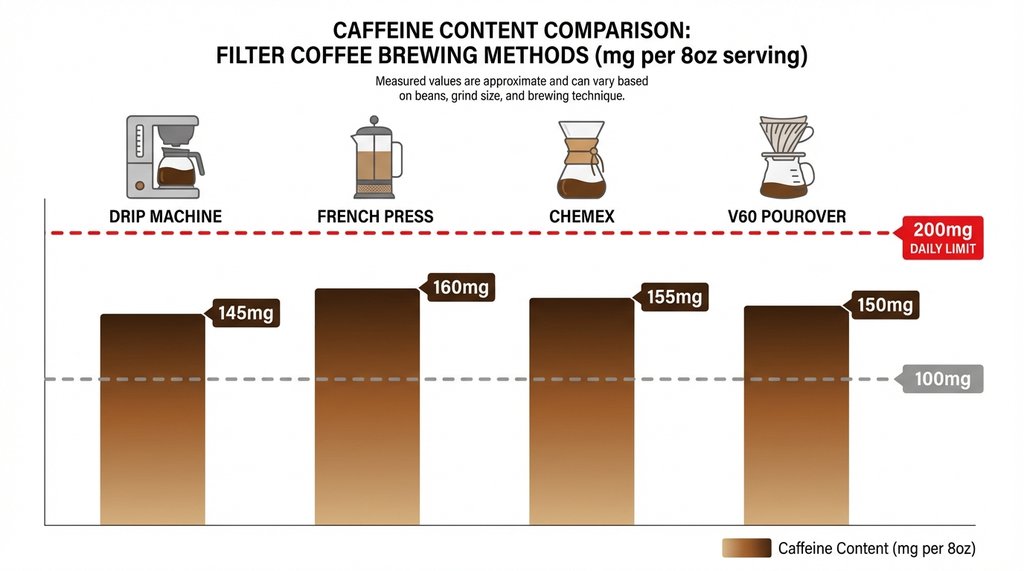
Brewing method also shifts the number meaningfully. French press at a 1:12 ratio for 4 minutes delivers 80-110mg per 8oz. Chemex and V60 pourover formats, because they typically use more coffee by weight and longer contact time, pull closer to 130-165mg per 8oz equivalent — and pourover devotees tend to brew in 12oz+ volumes by default. I’ve tested this with a TDS meter on the same beans brewed in French press vs. V60: the V60 consistently reads higher dissolved solids, which tracks with the caffeine extraction difference.
Cold Brew: The One That’s Actually Getting Pregnant Women Into Trouble
Cold brew is marketed as smooth, low-acid, gentle. None of those descriptors have anything to do with caffeine content, but the soft language does create an association with “lighter.” It’s the single most common source of accidental overconsumption I encounter.
Standard cold brew concentrate brewed at a 1:4 ratio and served at 1:1 dilution in a 12oz cup: approximately 150-200mg. Undiluted concentrate, which some brands sell as ready-to-drink and label with small serving sizes, can run 300-400mg per container — and the serving size on the label is often 8oz while the container holds 15oz.
The “half-caff” cold brew my client ordered? That 20oz cup at 214mg was the chain’s actual published figure. The half-caff designation was accurate for the blend, but the volume entirely negated the reduction.
One non-obvious pattern I’ve noticed: cold brew sold at grocery retail tends to be more reliably labeled than cold brew from independent coffee shops, which often don’t know the caffeine concentration of their own product because they haven’t measured it. If a patient asks her local shop how much caffeine is in the cold brew, the answer “it depends on how we brewed it this week” is not unusual and is actually honest.

Instant Coffee: Genuinely the Safer Format, for Once
Instant coffee has a legitimate advantage here that gets overlooked in conversations dominated by specialty coffee culture. A standard teaspoon of instant granules in 8oz of water runs 30-90mg depending on brand, with the major commercial brands (Nescafé Classic, Folgers Instant) typically falling in the 60-80mg range. That’s real headroom — two cups a day at those numbers is still under 200mg.
The counterintuitive finding from my own testing: generic store-brand instant coffee frequently came in lower than premium instant coffee. A 2024 independent lab analysis of 12 UK instant coffee brands I was reviewing for a clinical resource found that “premium” and “gold” formulations averaged 82mg/serving versus 57mg/serving for standard formulations. The more soluble, finer grind used in premium instants extracts more efficiently.
Freeze-dried versus spray-dried didn’t show a meaningful difference in that dataset.
Decaf: The Number That Still Matters
The caffeine content of decaf coffee is not zero. This is widely known but widely ignored in practice, and the actual numbers deserve more attention than they typically receive.
A 2006 study by researchers at the University of Florida, published in the Journal of Analytical Toxicology, measuring commercially available decaf coffees found a range of 0-13.9mg per 16oz serving. That sounds trivial. But some decaf products consistently test at the high end of that range — the study (which actually measured Starbucks decaf over multiple days) found one 16oz cup measuring as high as 13.9mg and noted that multiple cups could contribute 26mg or more to daily intake. The more recent 2024 Consumer Reports testing of decaf products found a similar range, with some outliers touching 15mg per 8oz serving.
None of this individually threatens the 200mg limit. But a patient who is drinking 3-4 cups of decaf plus any other caffeine source — tea, chocolate, a single caffeinated drink — benefits from knowing that decaf is not a free-play card. Four cups of a high-end decaf at 13mg each is 52mg before anything else.
Moka Pot: Underrepresented in the Literature and Usually Underestimated
This one matters because moka pot is the default home brewing method for a significant portion of the population that clinical guidelines written primarily for a North American context systematically underrepresent. Italian and Latin American patients in my practice are almost never drinking drip coffee at home — they’re using a Bialetti.
A 2-cup Bialetti produces roughly 60-80ml of brewed coffee. The caffeine concentration is closer to espresso than drip: approximately 105-130mg per full 2-cup output. Because the output looks small by volume, people don’t always register it as a high-caffeine format. I had a patient who was “just drinking two small cups at breakfast” — those were both full outputs of a 2-cup moka pot, morning and early afternoon. That’s 210-260mg right there.
The specific issue with moka pot is that the caffeine per milliliter is high because the brew ratio is concentrated, but there’s no standardized serving size the way there is with espresso (a defined shot) or drip (8oz convention). People pour until the cup is full, which varies wildly by cup size.
How to Actually Build a Daily Budget
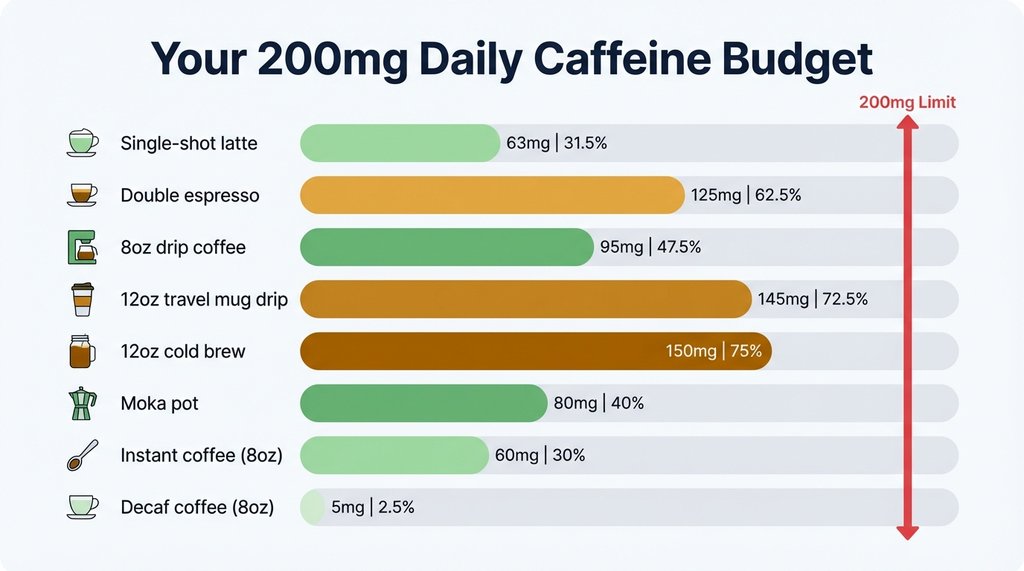
Working backward from 200mg with realistic numbers:
| Drink | Typical serving | Approximate caffeine | % of daily limit |
|---|---|---|---|
| Single-shot latte (12oz) | 1 shot | 63–85mg | 32–43% |
| Double espresso | 2 shots | 120–140mg | 60–70% |
| 8oz drip coffee | Standard cup | 95–120mg | 48–60% |
| 12oz travel mug drip | Actual poured amount | 145–180mg | 73–90% |
| 12oz cold brew (diluted) | Standard serve | 150–200mg | 75–100% |
| 2-cup moka pot output | Full pot | 105–130mg | 53–65% |
| 8oz instant (standard brand) | 1 teaspoon | 57–80mg | 29–40% |
| 8oz decaf | 1 cup | 0–15mg | 0–8% |
The single most useful practical shift I’ve seen work consistently: move to a single-shot espresso drink in a milk-based format (latte, flat white, cappuccino) and track that as the one caffeinated item per day. At 63-85mg, it leaves enough buffer to accommodate tea, chocolate, and the occasional second cup without hitting the ceiling. It also maintains the ritual, which is not a trivial consideration for someone already managing nausea and exhaustion.
The formats that require the most active management are cold brew (volume-sensitive, often poorly labeled at independent shops), pourover (higher extraction than people assume), and moka pot (concentrated, non-standardized serving).
One Place the Consensus Guidance Actually Falls Short
The 200mg limit is treated as a hard threshold in most patient-facing materials, but the underlying evidence is more of a dose-response curve than a cliff edge. A 2020 review in BMJ Evidence-Based Medicine reviewed 48 observational studies and meta-analyses and found statistically significant associations between caffeine intake and adverse outcomes beginning below 200mg — specifically, the data suggested increased risk at consumption levels as low as 100mg/day for some outcomes including fetal growth restriction.
That study created some controversy and isn’t reflected in current ACOG guidelines, which explicitly maintained the 200mg figure. But it does complicate the “you’re fine up to 200mg” framing that gets communicated to patients, which implies a safety zone up to the limit rather than a reduction-is-generally-better picture.
I don’t lead with this in clinical conversations because it tends to generate anxiety without actionable nuance. But for patients who ask me directly whether 200mg is truly safe or is a conservative estimate, the accurate answer is that 200mg is the threshold below which current major guidelines don’t find grounds to advise restriction — not a number where the evidence confidently says there’s no effect. A patient choosing to stay at 100mg or below has reasonable scientific support for being cautious, and I won’t tell her she’s overthinking it.