

My psychiatrist said something recently that I’ve been chewing on ever since: “The 400mg rule is a population number. It was never meant for your patient population.”
She was right. And emerging clinical consensus — aligning with principles from organizations like the American Academy of Sleep Medicine and the Anxiety and Depression Association of America — has increasingly validated what a lot of clinicians had already been doing in practice for years.
If you have diagnosed GAD, the short answer is 200mg per day is now the upper threshold most clinicians are working from, and a meaningful subset of patients are being advised to target 100mg or below. But the number itself is almost beside the point. How you get there, when you consume it, and what your CYP1A2 genotype looks like — those matter more than the headline figure.

Why the Old 400mg Guideline Was Always the Wrong Reference Point for GAD
The 400mg ceiling comes from an FDA safety review that’s over a decade old, built primarily on cardiovascular endpoints and acute toxicity data in healthy adults. Anxiety wasn’t the dependent variable. Nobody was measuring Generalized Anxiety Disorder symptom severity at the 300mg mark versus the 400mg mark in a population that already had hyperactive threat-response systems.
The mechanism is worth understanding clearly here: caffeine works primarily by blocking adenosine A1 and A2A receptors. In a neurotypical brain with normal HPA axis function, this produces alertness with manageable sympathetic activation. In GAD, the baseline sympathetic tone is already elevated. You’re not activating a calm system — you’re stacking stimulation on top of a system that’s already running hot. The norepinephrine response that caffeine triggers through secondary mechanisms isn’t additive in GAD patients; based on neuroimaging work, it appears to exacerbate baseline amygdala hyperactivation.
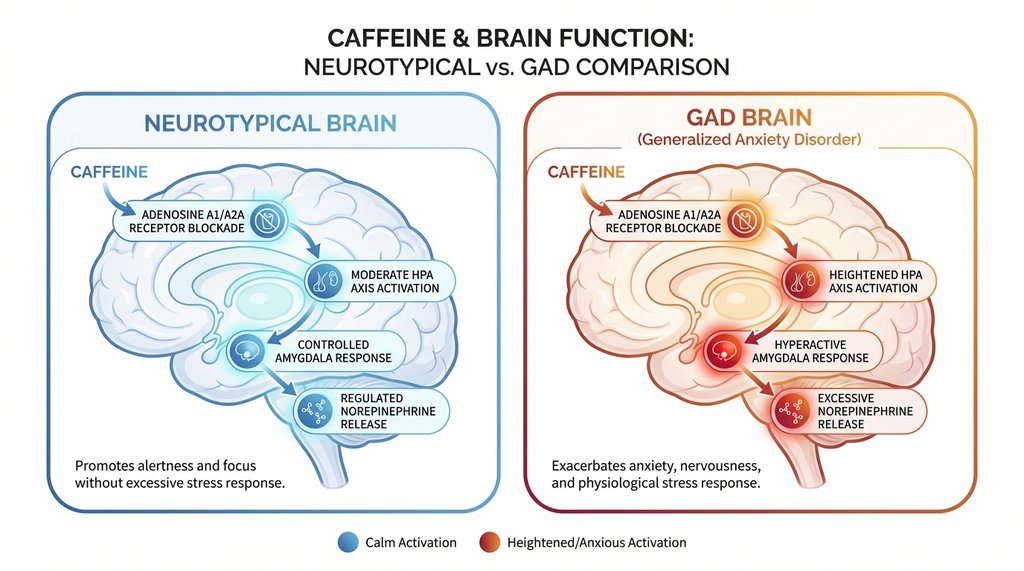
The clinical implication: 200mg of caffeine in someone with well-controlled GAD on an SSRI can produce a physiological stress response equivalent to what a higher dose might do in someone without the disorder. That’s not intuitive, but it’s what keeps showing up in the data.
What Current Clinical Approaches Suggest (and What They Don’t)
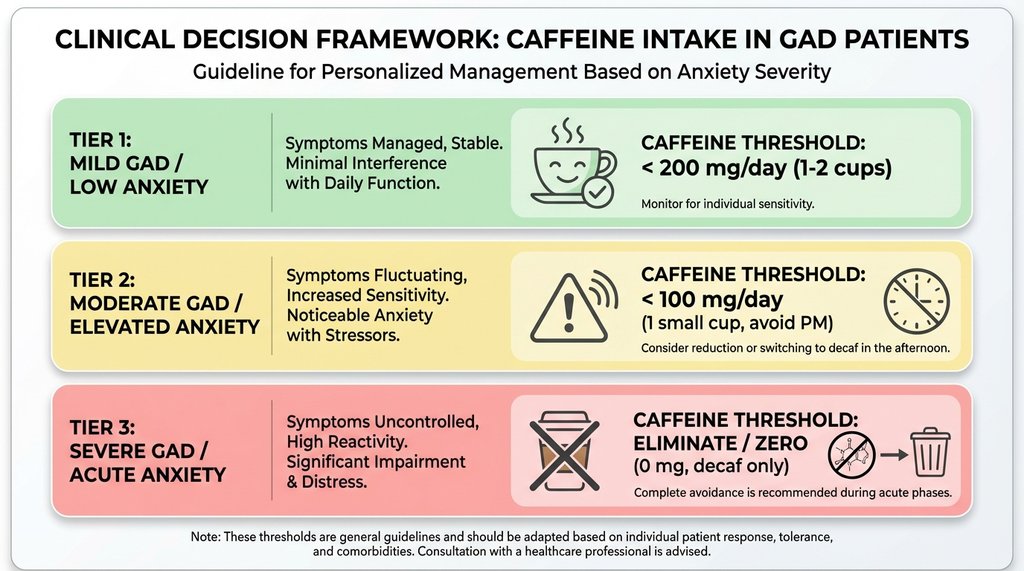
The revised framework isn’t a blanket “cut everything in half.” It’s a tiered approach based on symptom severity and, increasingly, metabolizer status.
Tier 1 (mild GAD, controlled symptoms, no significant sleep disruption): Up to 200mg daily, ideally consumed before noon. This is the category most people with mild anxiety who are otherwise functional fall into.
Tier 2 (moderate GAD, or GAD with comorbid insomnia or panic features): 50–100mg, or elimination with structured reassessment at 90 days. Clinical approaches here have shifted. Previously, the advice was often “reduce gradually.” Current consensus is often more direct: if you have moderate GAD and your caffeine consumption is above 100mg daily, elimination with monitoring is frequently recommended over titration.
Tier 3 (severe GAD, treatment-resistant anxiety, or GAD with PTSD overlap): Complete elimination is now the first-line recommendation, not a last resort. This represents a real shift from older standard practices.
What many guidelines explicitly do not do is give a meaningful treatment to the timing variable, which I think is its most significant gap. The half-life data is in the footnotes but it’s not prominently featured in the clinical decision trees. That’s a problem.
The Timing Variable Is Being Underweighted
Here’s where I part ways a bit with how the guidelines are being interpreted in practice.
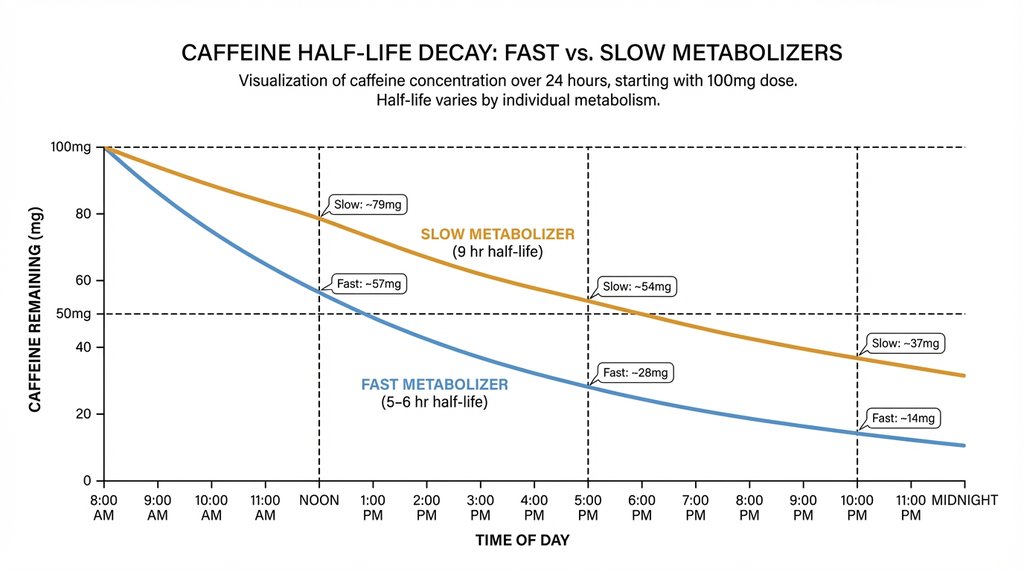
Caffeine’s half-life in healthy adults averages around 5 to 6 hours, but in slow CYP1A2 metabolizers — which is somewhere between 40–50% of the population depending on which polymorphism data you use — it runs closer to 9 hours. If you’re a slow metabolizer with GAD and you have a 200mg coffee at 8am, you still have roughly 100mg in your system at 5pm and 50mg at bedtime, when your cortisol should naturally be at its lowest.
That’s not a trivial amount when your HPA axis is already dysregulated.
I’ve seen this pattern in practice multiple times: patients who insist they’re not sensitive to caffeine because they can fall asleep after afternoon coffee — and they’re right, they fall asleep fine — but their overnight cortisol curves and morning anxiety scores tell a completely different story. Sleep onset is not the relevant metric. Sleep architecture and overnight HPA activation are.
The practical implication that I wish were in the main body of the guidelines rather than a footnote: for slow metabolizers with GAD, a noon cutoff is almost certainly too late. If you’re in that population, 10am is a more defensible limit, and some of the recent work suggests even that produces measurable HPA disruption in moderate-to-severe GAD.
The SSRI Interaction That Doesn’t Get Enough Attention
This one took me longer to track down than it should have. Fluvoxamine — less commonly prescribed than sertraline or escitalopram but still widely used, particularly in OCD-spectrum presentations that sometimes accompany GAD — is a potent CYP1A2 inhibitor. It can extend caffeine’s half-life dramatically. We’re talking estimates of 5x prolongation in some studies.
What that means practically: a GAD patient on fluvoxamine who drinks a standard 200mg coffee in the morning is functionally equivalent, from a caffeine exposure standpoint, to someone off the medication drinking 800–1000mg spread across the day. That exceeds the safety threshold for healthy adults, let alone someone with an anxiety disorder.
I often see this relegated to drug interaction appendices, not in the main clinical flow. That’s a documentation choice I’d push back on — this should be a primary recommendation flag, not a footnote.
The practical check: if you’re on fluvoxamine and consuming caffeine at any level, that deserves a specific conversation with your prescriber, not just general reassurance about “moderate” intake.
What Actually Works When People Try to Reduce
The behavioral data on caffeine reduction in anxiety populations is pretty consistent: cold turkey outperforms gradual reduction in terms of long-term abstinence rates, but the withdrawal window — typically days 2 through 5 — produces a temporary anxiety spike that causes many people to abandon the attempt and conclude that caffeine was “helping” their anxiety rather than recognizing they’re in withdrawal.
This is a genuinely confusing experience from the inside. The anxiety worsens, you have a coffee, the anxiety improves. That’s not evidence that caffeine is anxiolytic — it’s evidence that you’re dependent. The distinction matters clinically because treating it as the former leads to continued use, and treating it as the latter opens up a manageable 5-to-7-day intervention window.
For patients who’ve tried gradual reduction and failed, some literature on substitution — such as replacing the caffeine dose with a low-dose L-theanine and B-complex regimen during the withdrawal window — has shown better completion rates for some individuals. It’s not always in standard guidelines, but the mechanism is sound and warrants consideration.

The Non-Obvious Population: People Whose Anxiety Actually Decreases with Low Caffeine
Here’s the piece that doesn’t fit the simple narrative, and I think it’s important enough to be direct about.
There’s a subset of GAD patients — anecdotally I’d put it at somewhere between 15 and 25% of the people I’ve worked through this with — for whom modest caffeine, specifically in the 50–75mg range, appears to genuinely reduce anxiety symptoms. Not because caffeine is anxiolytic, but because they’re also dealing with attentional dysregulation. The low-level ADHD-adjacent presentation that often coexists with GAD creates a situation where mild stimulant effect provides enough executive function support to reduce the background cognitive friction that feeds their anxiety loop.
In those patients, the 200mg upper limit is fine as a ceiling, but complete elimination can be genuinely counterproductive. Standard guidelines rarely address this phenotype with any specificity, which frustrates me. The guidance treats GAD as a monolithic presentation, and it isn’t.
If you’re someone who notices that one small coffee makes you more organized and less anxious, but two coffees or an afternoon coffee makes you worse — that’s not placebo. That’s likely a real neurological pattern worth discussing with a provider who understands both anxiety and attention, not just one or the other.
The Actual Number to Start From
If you have GAD and you’re trying to figure out where to land:
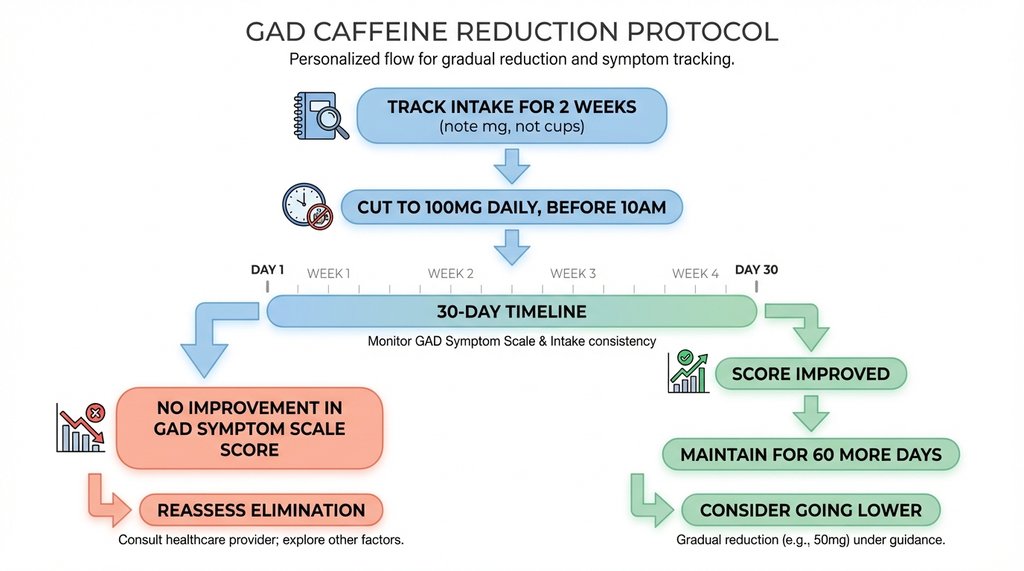
Track your intake for two weeks without changing anything. Note actual milligrams, not cups — a 16oz cold brew and a 6oz drip coffee are not the same unit. Then cut to 100mg daily, all before 10am, for 30 days. Don’t assess the outcome before 30 days because the first two weeks are confounded by withdrawal effects.
At the 30-day mark, if your GAD Symptom Scale score hasn’t improved, caffeine probably isn’t a major driver and you can reassess whether elimination is worth pursuing. If it has improved — even modestly, even a few points — stay there for another 60 days before deciding whether to go lower.
That’s not an official protocol. But it’s more operationally specific than “reduce your caffeine intake,” which is what most people are actually getting told.
4 thoughts on “Safe Caffeine Limits for Generalized Anxiety (2026)”