

My patient — I’ll call her M., a 47-year-old software architect — came in holding a printed-out Reddit thread and a three-page spreadsheet she’d built tracking her heart palpitations against her daily coffee intake. She’d been doing this for six weeks. The timestamp precision was genuinely impressive. What the spreadsheet couldn’t tell her was whether her 380mg daily habit was the actual problem, or whether the anxiety disorder she’d been managing for nine years was amplifying signals that a different person’s cardiovascular system would have simply ignored. That distinction matters enormously, and most caffeine advice online collapses it into a single number — usually “400mg is fine” — and moves on.
That’s the wrong answer for a significant portion of coffee drinkers.

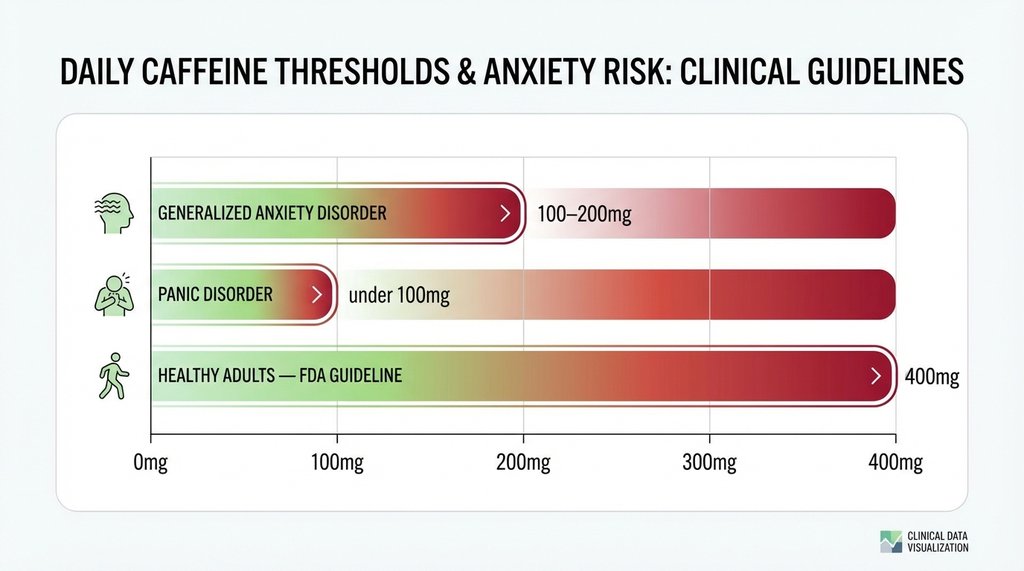
The 400mg Figure Is a Population Average, Not a Safety Threshold
The FDA’s 400mg-per-day guideline comes from studies on healthy adults without pre-existing conditions. It’s a reasonable upper bound for a hypothetical median person. But it was never calibrated for generalized anxiety disorder, panic disorder, atrial fibrillation, hypertriglyceridemia, or any of the other conditions that dramatically change how caffeine interacts with your physiology.
What the research actually shows, broken down by condition:
For anxiety disorders (GAD, panic disorder, social anxiety): The threshold where caffeine reliably worsens symptom frequency and severity in clinical populations sits significantly lower — around 100–200mg per day for most patients, and below 100mg for those with panic disorder specifically. Recent clinical reviews suggest that even moderate caffeine intake (200–300mg) increases self-reported anxiety scores in GAD patients. While the numerical increase on clinical rating scales might sound small, in practice it’s the difference between a manageable day and one where a patient is rescheduling meetings because they can’t stop the spiral.
The mechanism isn’t mysterious: caffeine antagonizes adenosine receptors and simultaneously spikes cortisol and adrenaline. For someone whose baseline sympathetic nervous system tone is already elevated — which describes most people with clinical anxiety — you’re adding fuel to a fire that’s already burning higher than it should be.
For cardiac arrhythmias (specifically AFib): This is where the data gets genuinely interesting, and where a lot of cardiologists are now walking back older, more restrictive advice. For years, patients with atrial fibrillation were told to eliminate caffeine entirely. The current evidence doesn’t support that blanket recommendation.
A 2021 observational study out of UCSF (Kim et al.) analyzed data from over 386,000 individuals and found no evidence that coffee consumption increases the risk of arrhythmias. In fact, each additional daily cup of coffee was associated with a 3% lower risk of incident arrhythmias, including AFib. Patients with lone AFib (normal heart structure, no underlying disease) showed almost no measurable increase in risk even at higher intakes.
The clinical takeaway: AFib itself is not a categorical reason to eliminate caffeine. Whether your AFib warrants restriction depends on whether you have structural heart disease underneath it.
For hypertension: 200mg of caffeine raises systolic blood pressure by roughly 3–4 mmHg in habituated drinkers, more (8–10 mmHg) in non-habituated individuals or those with certain genetic variants affecting CYP1A2 metabolism. For most people with well-controlled hypertension, this is clinically irrelevant. For someone already sitting at 145/90 on medication, that spike matters more. The number I use with patients as a working upper bound here is 200mg/day, with a 6-hour cutoff before bed.
The Genetic Variable Nobody Is Talking to Patients About
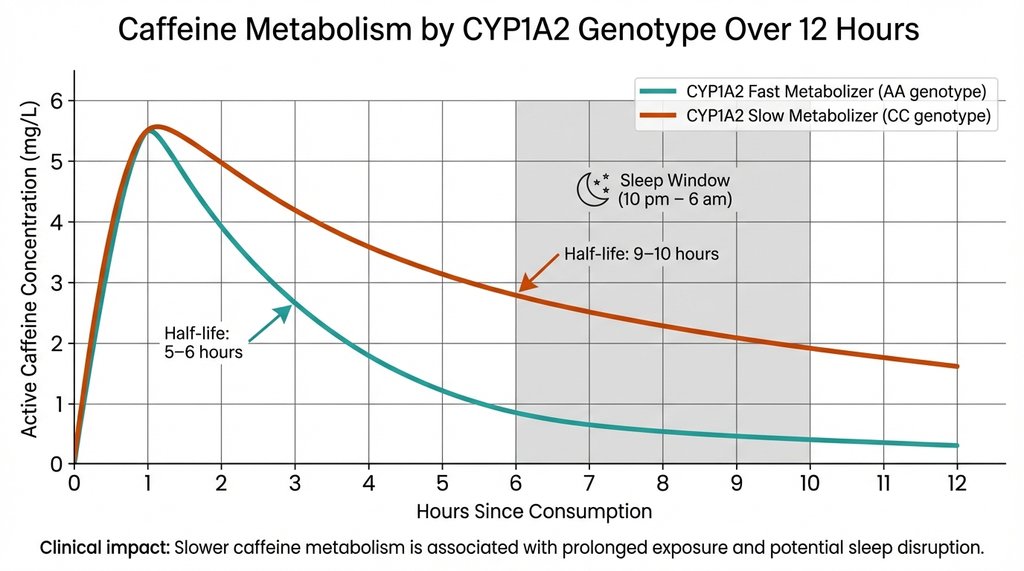
CYP1A2. This enzyme, encoded by the CYP1A2 gene, is responsible for roughly 95% of caffeine metabolism in your liver. Fast metabolizers (the AA genotype) clear caffeine at approximately twice the rate of slow metabolizers (the CC genotype). For reference: in slow metabolizers, caffeine’s half-life extends from the typical 5–6 hours up to 9–10 hours. This metabolic rate can further slow down due to hormonal changes like declining estrogen.
This is not a trivial difference. A slow metabolizer drinking 200mg of caffeine at noon still has roughly 100mg active in their system at 10pm. That residual load feeds directly into sleep architecture disruption, and disrupted sleep independently worsens both anxiety symptoms and cardiac arrhythmia frequency. I’ve had patients cut their caffeine to what seemed like a medically conservative level — 150mg before noon — and still report worsening insomnia and anxiety. When we looked at their genotype, they were homozygous slow metabolizers. The fix wasn’t just reducing dose; it was moving the dose earlier and getting below 100mg total.
Consumer genetic testing through companies like 23andMe reports CYP1A2 status if you dig into the raw data (it’s not in the standard health report). Alternatively, a simple empirical test: if you’re caffeine-sensitive to an unusual degree, or if you can drink coffee at 4pm and still fall asleep fine, your metabolism is telling you something your bloodwork won’t.
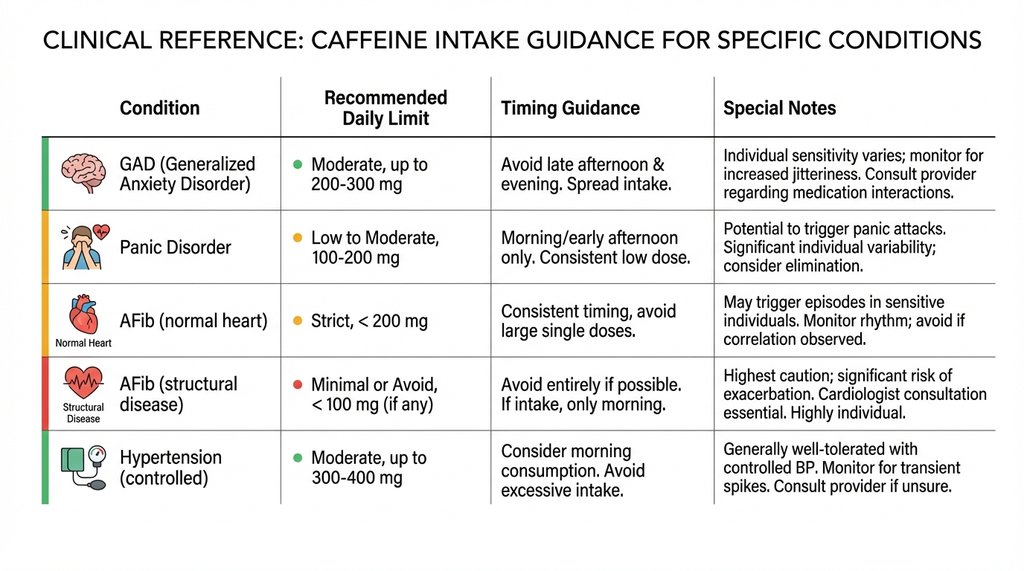
The Specific Numbers I Use With Patients, By Category
These are working guidelines, not fixed rules — every one of them needs to be calibrated against individual response.
Generalized Anxiety Disorder (without panic):
- Starting conservative target: 100–150mg/day
- Administered as a single morning dose before 10am
- No dose on high-stress days (the anxiety amplification effect is additive)
- If symptom improvement is meaningful at 8 weeks: maintain. Do not titrate back up experimentally without clear reason.
Panic Disorder:
- My honest recommendation: below 50mg/day, or elimination entirely during active treatment phases
- Even 100mg can precipitate panic attacks in sensitized individuals, because the physical sensations of caffeine — elevated heart rate, slight chest tightness, warmth — are often identical to the early somatic cues that trigger the panic cycle
- This is the one condition where I genuinely think most patients do better without caffeine than with even small amounts. The taste ritual can be maintained with half-caff or herbal alternatives.
AFib (structurally normal heart):
- 200–300mg/day is generally defensible
- Strong preference for morning-only dosing
- If patient also has anxiety: apply anxiety guidelines, not the cardiac ones — the lower number wins
AFib (with structural disease, reduced EF, or significant left atrial enlargement):
- Under 200mg/day, with ECG monitoring if they want to maintain regular intake
- Holter monitor data is more useful here than symptom diaries — patients consistently undercount palpitation episodes
Hypertension (controlled, on medication):
- 200mg/day upper limit
- No caffeine within 30 minutes before BP is normally taken (this skews readings in a way that has caused patients to have their medications unnecessarily adjusted)
Where Most Online Advice Gets It Wrong for This Population
The advice to “listen to your body” is repeated constantly and is, for anxiety patients specifically, actively counterproductive. People with anxiety disorders are not underresponsive to bodily signals. They are dramatically overresponsive. Telling someone with GAD or panic disorder to use self-monitoring as their primary guide is like telling someone with hyperalgesia to rate their pain on a 1–10 scale and adjust accordingly — the calibration is off in a way that will systematically produce overly conservative or overly catastrophizing responses.
What actually works: structured dose reduction (cut by 25% every 10 days, not cold turkey), morning-only timing, and tracking sleep quality as a proxy metric rather than anxiety symptoms directly, because sleep quality is more objective and less prone to the catastrophizing distortion.
Cold-turkey caffeine elimination also, counterintuitively, can worsen anxiety short-term. Withdrawal headaches and fatigue activate the same threat-detection system that anxiety disorder already keeps on high-alert. I’ve had patients who eliminated caffeine over a weekend, felt terrible for three days, concluded their anxiety was “not caffeine-related,” and reinstated their full intake — when in fact they’d just run into withdrawal, not evidence of anything.
On the Decaf Question
Decaf is not zero caffeine. An 8oz cup of drip decaf typically contains between 2–15mg of caffeine depending on the bean and decaffeination method. Swiss water process decaf is generally on the lower end (often under 2mg per cup). Standard commercial solvent-process decaf runs higher, typically 2–15mg. For most people, that’s irrelevant. For a slow CYP1A2 metabolizer with panic disorder drinking three decafs a day, it adds up to a real dose.

What I Actually Told M.
Her spreadsheet showed a clear signal: palpitations spiked consistently on days when she consumed caffeine after 1pm and on days where her total intake exceeded 320mg. Below 250mg, morning-only, the frequency dropped substantially. Her anxiety was still present but not clearly correlated with the caffeine variable in her own data — she’d actually done a good enough experiment to separate the two, which is more than most patients do.
The recommendation: cap at 200mg, before noon, track for another six weeks. If the palpitations resolved meaningfully — which they did — consider requesting a CYP1A2 panel if she wanted to understand the mechanism. She did. She was a slow metabolizer. The 1pm coffees she’d been having were still 60–70% active in her system at midnight. The fix was obvious once you had that number.
That’s the difference between population-level caffeine guidance and an answer that’s actually calibrated to a specific person’s cardiovascular and neurological reality. The 400mg headline will always be wrong for some meaningful fraction of the people reading it.
2 thoughts on “Safe Caffeine Limits for Anxiety & Heart Conditions”